


What is a pterygium?
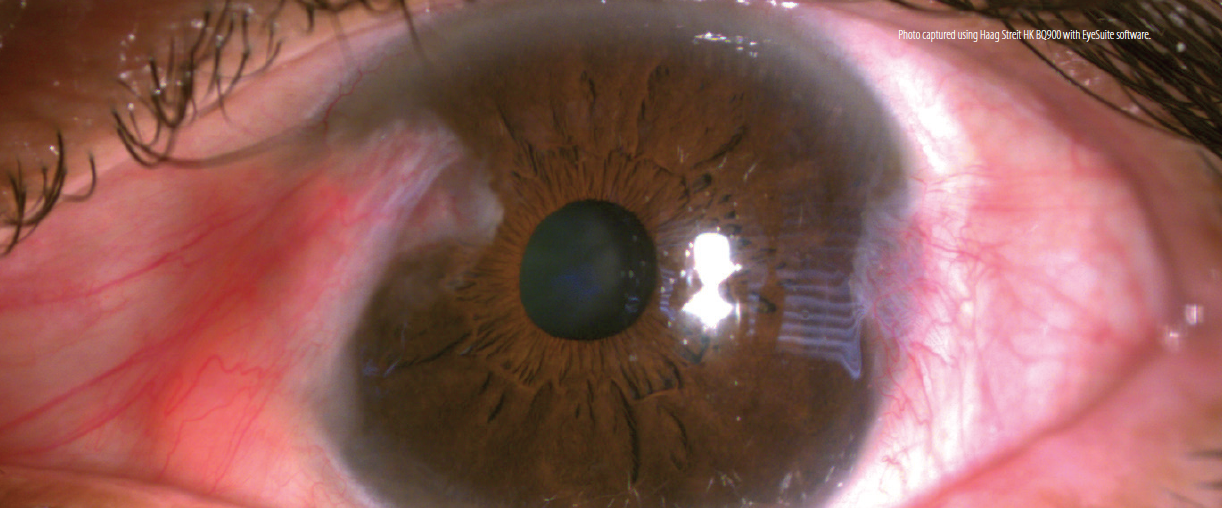
A 46-year-old Hispanic woman presented with complaints of mild vision blur, constant burning, hyperemia, and ocular irritation in her left eye for the past week. Her symptoms had been worsening since she started her new job as an agricultural worker harvesting strawberries. BCVA was 20/20 OD and 20/25 OS. The patient had 0.75 D of irregular astigmatism OS, and her anterior segment examination was significant for blepharitis, meibomian gland dysfunction (MGD), and ocular surface disease (OSD) in each eye. Notably, there was a temporal and nasal (double) pterygium in her left eye (Figure).
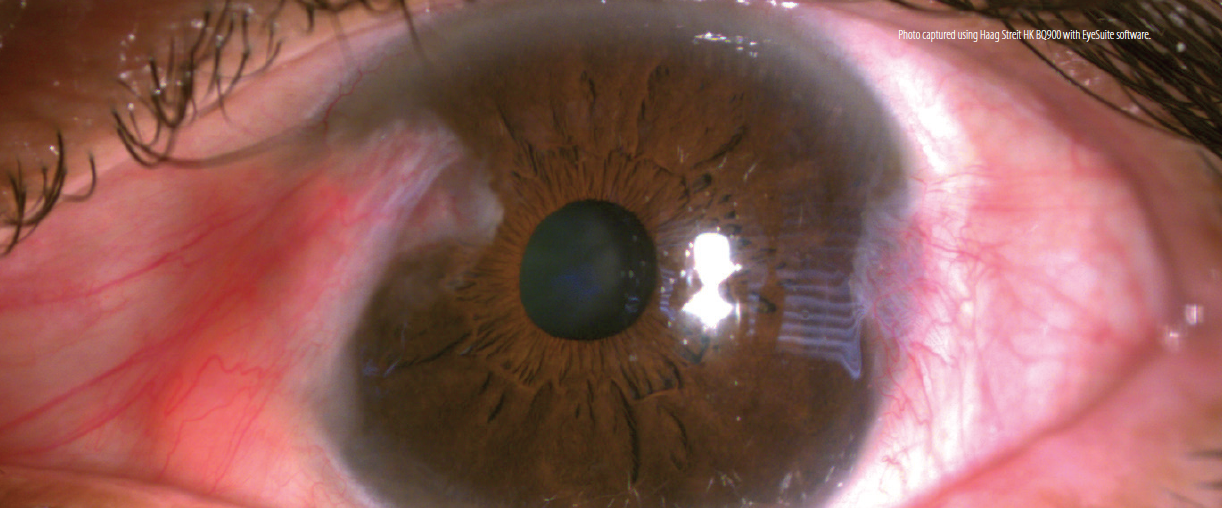
(Photo captured using Haag Streit HK BQ900 with EyeSuite software.)
Tear osmolarity findings were 332 mOsm/L OD and 354 mOsm/L OS, indicating the presence of hyperosmolar tears. Matrix metallopeptidase 9 (MMP-9) testing yielded a strongly positive result (> 40 ng/dL) OU. Corneal staining was grade 1+ OD and grade 2+ OS. Previous treatments with artificial tears and warm compresses had not been helpful, according to the patient.
DISCUSSION
Pterygium (aka surfer’s eye) is a subepithelial fibrovascular growth of degenerative nature that originates on the temporal and/or nasal bulbar conjunctiva and extends onto the cornea. The exact etiology of pterygium is unknown, although it has been highly associated with climatic UV radiation. Other risk factors include increasing age, living in a geographical lower latitude, and working outdoors in a rural area. The prevalence of pterygium is 10.2%, with a slight preponderance in men.1,2 A 2019 study reported that eyes with pterygium have increased tear osmolarity, reduced tear breakup time, reduced Schirmer testing, more corneal staining, and reduced tear meniscus height compared with normal eyes.2 These factors all contribute to OSD.
The patient was treated with loteprednol etabonate ophthalmic gel 0.5% (Lotemax Gel, Bausch + Lomb) twice daily and lifitegrast ophthalmic solution 5% (Xiidra, Novartis) twice daily to decrease the inflammatory response on the ocular surface. Microblepharoexfoliation and vectored thermal pulsation were performed for the presence of blepharitis and MGD. Use of UV protection outdoors was also emphasized to the patient, especially when at work. She decided to defer surgical treatment, continue lifitegrast, and monitor symptoms.
Source
https://modernod.com/articles/2020-sept/pterygium?c4src=article:infinite-scroll

All Eye
Care Services

Keep
In Touch
MAP
© 2025 Avant Eyes Optometry. All Rights Reserved. Accessibility Statement - Privacy Policy - Sitemap
Powered by: 